Bahagian 2: Lebih Daripada Sekadar Luka Biasa: Otitis Eksterna, Malignant Otitis Eksterna (MOE) Dan Perikondritis.
Jul 08, 2026

October 30 2025
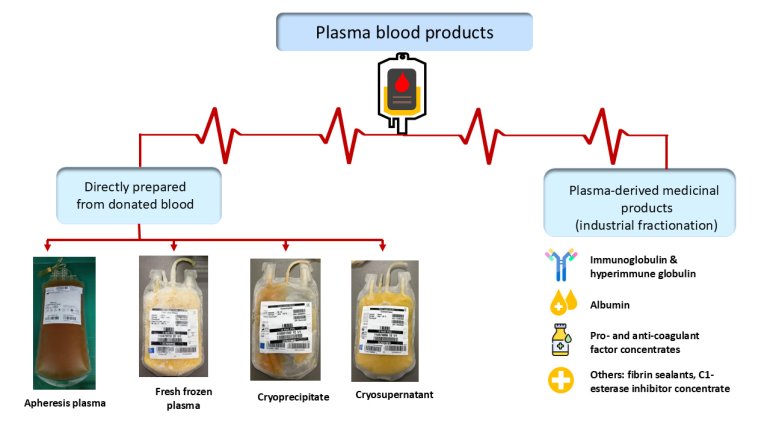
Plasma is a vital part of transfusion medicine and is one of the three main components of blood, along with red cells and platelets. It is the liquid portion of blood, made up of about 90% water and 10% solutes. It contains vital proteins such as albumin, clotting factors, and immunoglobulins. Plasma constituents are essential in maintaining blood volume, osmotic balance, coagulation, and immune defence.
Types and clinical indications of plasma products
1. Fresh frozen plasma
Fresh frozen plasma (FFP) is a component that contains labile clotting factors and other constituents, for transfusion or fractionation. FFP can be obtained directly by plasmapheresis or isolated from whole blood donations through centrifugation. If FFP is obtained from whole blood donation, the duration of whole blood donation shall not exceed 15 minutes, and FFP should be prepared within 24 hours. FFP is stored frozen at below -25ºC for up to three years, and it must be thawed at temperature of 37°C before use, with a post-thaw shelf life of 24 hours when stored at 1–6°C (1). It contains all coagulation factors at normal levels. FFP is indicated for patients with multiple coagulation factor deficiencies, massive transfusion, disseminated intravascular coagulation, liver disease, and urgent warfarin reversal when prothrombin complex concentrate (PCC) is not available.
2. Cryoprecipitate
Cryoprecipitate is a blood component that contains fibrinogen, fibronectin, factor VIII, von Willebrand factor, and factor XIII, which is obtained by thawing and further processing of FFP. Cryoprecipitate is stored frozen at below -25ºC for up to three years, and it is thawed at temperature of 37°C before use. As fibrinogen is the first clotting protein to drop to critically low levels during significant bleeding, replacing low fibrinogen in haemorrhage is now the primary indication for cryoprecipitate transfusion. Such conditions include inherited or acquired fibrinogen hypofibrinogaemia or dysfibrinogenaemia with bleeding (2).
3. Cryosupernatant
Cryosupernatant is a by-product of the preparation of cryoprecipitate. It consists of plasma component that has been depleted of factor VIII, fibrinogen, fibronectin, and factor XIII. Similar to other plasma products, cryosupernatant is stored frozen at below -25ºC for up to three years, and it must be thawed at temperature of 37°C before use (1). Cryosupernatant is used for plasma exchange in thrombotic thrombocytopenic purpura or haemolytic-uraemic syndrome.
4. Plasma-derived medicinal products (PDMPs)
Plasma-derived medicinal products (PDMPs) are produced from pooled plasma through fractionation, which separates and purifies specific proteins into stable, concentrated therapeutic preparations. Currently, around 30 proteins are suitable for manufacturing into PDMPs, with the most common being albumin, immunoglobulins, and coagulation factor concentrates.
Treatments utilising PDMPs can be categorised into four distinct types: replacement or substitution therapies involving products such as pro- and anti-coagulant factor concentrates (factor VIII concentrates, factor IX concentrates), polyvalent immunoglobulin, specific or hyperimmune globulin (hepatitis B immunoglobulin, rabies immunoglobulin, anti-D immunoglobulin), albumin, alpha 1-antitrypsin, fibrin sealants, and C1-esterase inhibitor concentrate; immune-modulating therapies (polyvalent IgG, alpha 1-antitrypsin); anti-inflammatory therapies (polyvalent IgG, anti-thrombin, activated protein C); and therapies targeting plasma protein antagonist functions (PCC, activated PCC). These and other PDMPs are essential for the prevention and treatment of patients with bleeding disorders, immunological deficiencies, autoimmune and inflammatory diseases, and many congenital deficiency syndromes (3).
Safety, Supply, and Long-Term Use
Plasma products are much safer now than they were during the viral transmission crises of the 1980s. Strict donor screening, nucleic acid testing, and several steps to eliminate pathogens, such as the use of riboflavin or psoralens as pathogen inactivation techniques, make plasma transfusion one of the safest medical procedures. In PDMPs production, solvent/detergent treatment, pasteurisation, nanofiltration, and ultraviolet-based pathogen inactivation have significantly enhanced viral reduction, ensuring an exceptionally high safety level by effectively inactivating or eliminating both enveloped and non-enveloped viruses, thereby minimising the risk of viral transmission (3).
Despite these advances, global plasma supply remains uneven, heavily reliant on a few countries. The World Health Organization advocates for regionally self-sufficient plasma programs supported by voluntary, non-remunerated donors to ensure equitable access and ethical sustainability (4).
In Malaysia, the Ministry of Health is strengthening national plasma collection and fractionation capacity under its strategic roadmap. Achieving self-sufficiency requires continued collaboration among all blood transfusion services in the nation to optimise donor recruitment, enhance quality assurance, and ensure judicious clinical use of plasma products.
References
Transfusion Practice Guidelines for Clinical and Laboratory Personnel. National Blood Centre, Ministry of Health, Malaysia. 4th edition, 2016.
Wong H, Curry N. Cryoprecipitate transfusion: current perspectives. International Journal of Clinical Transfusion Medicine. 2016;22:89-97.
Strengers PF. Challenges for plasma-derived medicinal products. Transfusion Medicine and Hemotherapy. 2023;12;50(2):116-22.
World Health Organization. Global Database on Blood Safety: Plasma-Derived Medicinal Products. Geneva: WHO; 2022.