Dr Seethala Devi A/P Marathamuthu, Dr Sharmila A/P Manian and Dr Siti Salmah binti Noordin
Kluster Perubatan Regeneratif
In December 2019 the World Health Organization (WHO) was awakened to a COVID-19 infectious outbreak that took place in the Hubei Province of China. Overnight, the healthcare system all over the world was facing a big challenge on accommodating and giving care to the rapidly increasing patient load in hospitals. In the beginning, the management for COVID-19 was mainly supportive treatment while the researchers and clinicians diligently continue to investigate and implement a variety of therapies alongside creating vaccine to combat this pandemic. Joining the bandwagon is also the usage of plasma from the convalescent donors to treat patients with severe COVID-19 infections. This therapy is called convalescent plasma (CP) therapy.
This interesting method of treatment is not foreign in the medical fraternity as the blood products from the recovered patients have been used since the late 1800s. Convalescent plasma therapy is mostly a choice of treatment for infectious diseases that generally lacks vaccine and therapy with a highly infectious nature of virus and high case of fatality rate. This therapy was used during emerging infectious diseases like the West African Ebola outbreak, West Nile Virus, MERS-CoV, SARS-CoV-1, and H1N1.
Before diving in-depth into the CP therapy topic, let us be familiarized with the terms being used. Convalescent means that a person is recovering after an illness or medical treatment. Plasma is a light amber liquid component of blood that is freed from blood cells but holds proteins and other constituents of whole blood in suspension. Plasma makes up about 55% of blood’s total volume. Hence, CP therapy in COVID-19 simply means using plasma from patients who have recovered from COVID-19 and transfusing it to the newly exposed patients to confer temporary immunity and may this help in reducing the viral load. The goal of antibodies in this treatment is to kill the virus and prevent additional replication as well as disease-related tissue damage.
People who have been clinically recovered from COVID-19 infection and tested negative for SARS-CoV-2 by polymerase chain reaction (PCR) technique are considered donors for CP. Patients with COVID-19 can be divided into two groups: symptomatic and asymptomatic. For symptomatic patients, clinical recovery is defined as the absence of fever for at least 24 hours and improvement in respiratory symptoms such as cough and shortness of breath for at least 10 days. The clinical recovery time for asymptomatic individuals is 10 days following the initial positive oropharyngeal swab or nasopharyngeal swab. Physicians will choose potential CP donors who are clinically asymptomatic at least one week after discharge, and these donors will be tested for COVID-19 immunoglobin (Ig) G antibody as well as other screening tests that are required, such as HIV, Hepatitis B, Hepatitis C, and syphilis screening, full blood count, liver function test, and SARS-CoV-2 antibody test.
Before CP donation, pre-donation counseling will be conducted to all donors. The potential donors are counseled about the donation process and possible donor adverse reactions. During counseling, review of SARS-CoV-2 PCR and antibody results are also made.
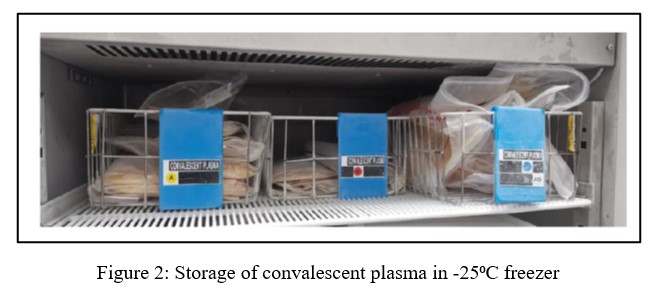
The CP donation can be made via whole donation and apheresis. However, apheresis donation is recommended as it can obtain a higher volume of plasma collection around 400- 500 mL. Following collection, the donated plasma components will be labeled as CP and kept frozen at or below -25°C while waiting for the transfusion microbiology results. The CP unit will be stored at the blood centers in a separate designated blood bank freezer up to 24 months. Once the request for the CP plasma is received, the appropriate ABO blood group matched CP unit for transfusion will be selected. Convalescent plasma that is transported as liquid plasma will have the temperature maintained between 2-6°C and it can be stored up to 40 days, while CP that is transported in frozen state (– 25°C) can be stored up to 24 months.
The selection of CP recipient is also done meticulously by the attending physician. Written consent for CP treatment is obtained from the donor before its administration. Current indications for CP treatment include laboratory-confirmed COVID-19 infection with severe or critical illness who are admitted to Intensive Care Unit and on ventilation, patients with myocarditis or myocardial dysfunction due to SARS-CoV-2 infection, and patients with hemophagocytic lymph histiocytosis (HLH) secondary to SARS-CoV-2 infection. The CP treatment is also considered in COVID-19 patients who are predicted for progression to severe illness. This treatment is contraindicated in patients with a history of severe or life-threatening allergic reactions to blood or plasma products and patients with underlying Ig A deficiency. The recommended standard dose of CP treatment for an adult is approximately 200-250 mL as a single dose over 1-2 hours transfusion while 4-5 mL/kg as a single dose over 1-2 hours transfusion for children. The most common risks linked with CP therapy include febrile non-hemolytic reaction, allergic reaction, transfusion-associated circulatory overload (TACO), and transfusion-related acute lung damage (TRALI), which are all common with standard plasma transfusion.
Previous clinical trials of CP treatment had been shown to relieve clinical symptoms in moderate to severe COVID-19 patients especially if the CP had a high-titer of viral neutralization antibody and high levels of antibody Fc-mediated function. However, recent evidence has shown that CP treatment does not improve risk of intubation or death at 30-day. Furthermore, CP treatment is also not recommended in non-severe COVID-19 patients. Thus, additional studies are needed to assess the effectiveness of CP therapy among different types of patients’ populations as well as its optimal dose.
Figure 1: A unit of frozen convalescent plasma
Penulis Artikel
Nama penulis:
Dr Seethala Devi a/p Marathamuthu, Dr Sharmila a/p Manian dan Dr Siti Salmah binti Noordin
Afiliasi:
Kluster Perubatan Regeneratif
Bidang kepakaran:
Transfusi Perubatan.